You know those moments when a patient describes feeling lightheaded, maybe getting a bit sweaty, and then suddenly needing to sit down? These experiences offer us an incredible opportunity to demonstrate the power of neurologically-focused assessment and care.
When a patient experiences a vasovagal episode, it opens the door to a deeper conversation about their nervous system function and adaptive capacity.
The reality is striking—research has found that approximately 1 million Americans experience a syncope episode every year, with more than 80% of episodes of syncope being vasovagal. Yet most conventional approaches focus solely on the cardiovascular aspects, overlooking the critical neurological component that’s at the heart of these episodes.
Let’s be real—most practitioners are taught to view vasovagal episodes as simply “the common faint” without appreciating how they reflect information about a patient’s autonomic nervous system function and adaptive capacity. When we reduce these episodes to merely a cardiovascular event, we miss the opportunity to address the underlying neurological dysregulation.
Vasovagal episodes represent a window into autonomic nervous system function—specifically, how well the sympathetic and parasympathetic systems are balanced. When we understand these episodes through the lens of neurological function, we can move beyond simply managing episodes to improving the patient’s overall nervous system regulation and resilience.
The Neurophysiology of Vasovagal Episodes
Vasovagal syncope is fundamentally a neurological event masquerading as a cardiovascular problem. It represents the most common form of reflex syncope, accounting for over 85% of syncopal events in people younger than 40 years. At its core, it results from a temporary failure in the autonomic nervous system’s regulation, a drop in blood pressure, and heart rate, leading to reduced cerebral perfusion and loss of consciousness.
The key to understanding these episodes lies in recognizing them as a reflex arc with both afferent and efferent limbs. When triggered, the afferent limb sends signals to the central nervous system that initiate neurological events. The central nervous system then responds through the efferent limb with two critical actions: increased parasympathetic activity and heightened vagal tone, combined with decreased sympathetic activity that reduces vascular tone. This neurological double-hit dramatically reduces cardiac output and blood pressure, causing insufficient blood flow to the brain.
In patients prone to vasovagal episodes, we often see evidence of autonomic dysregulation that creates vulnerability. This dysregulation can manifest as:
- Exaggerated parasympathetic responses to certain triggers
- Inadequate sympathetic tone to maintain blood pressure during challenges
- Poor coordination between the two branches of the autonomic system
- Reduced overall adaptive capacity or “autonomic reserve”
Technical Breakdown of Vasovagal Episodes
To fully appreciate vasovagal episodes from a neurological perspective, we need to examine the distinct phases and components that make up these events.
The Three Phases of a Vasovagal Episode
- Trigger Phase: The cascade begins with a trigger that activates the afferent limb of the vasovagal reflex. This trigger, combined with central hypovolemia, activates mechanoreceptors in the ventricle that signal through vagal afferents to the central nervous system.
- Physiological Response Phase: Once triggered, the efferent limb produces a two-pronged neurological response: increased vagal firing causes a significant decrease in heart rate, while decreased sympathetic activity leads to reduced vascular tone. This drops mean arterial pressure below the threshold where cerebral autoregulation can maintain adequate blood flow.
- Recovery Phase: When the patient falls or is placed supine, the increased circulating blood volume from the lower extremities combined with the reduced gravitational challenge allows rapid restoration of blood flow to the brain and recovery of consciousness.
Common Triggers Categorized by Neurological Impact
Triggers for vasovagal episodes vary widely but can be categorized based on how they impact the nervous system:
Emotional/Psychological Triggers:
- Fear, anxiety, or intense emotional stress
- The sight of blood, needles, or injury
Physical/Postural Triggers:
- Prolonged standing, especially in warm environments
- Sudden positional changes
- Dehydration or reduced blood volume
Situational Triggers:
- Intense pain
- Coughing, sneezing, or straining
- Urination (particularly in men)
Prodromal Symptoms and Autonomic Signaling
Most patients experience warning signs before losing consciousness—a critical window for intervention:
- Lightheadedness and dizziness
- Nausea
- Pallor and cold, clammy skin
- Visual changes like tunnel vision
- Weakness or fatigue
These reflex syncope symptoms aren’t random—they’re direct manifestations of specific autonomic nervous system changes that precede the full vasovagal episode.
Comparative Analysis: Beyond the Traditional Approach
When it comes to vasovagal attacks, the conventional medical model and a nervous system-focused approach represent fundamentally different paradigms in assessment and management.
Conventional Medical Approach:
- Focuses primarily on the fainting event itself
- Relies heavily on patient history and symptom description
- Uses tests like orthostatic blood pressure and Electrocardiogram (ECG)
- Aims to exclude dangerous causes rather than understand the underlying function
Nervous System-Focused Approach:
- Examines the broader context of autonomic nervous system function
- Utilizes objective measurements of neurological and autonomic balance
- Employs advanced technologies to assess Heart Rate Variability
- Aims to understand the patient’s unique autonomic signature and adaptive capacity
The diagnostic tools employed in these two approaches reveal another important contrast:
Conventional Diagnostic Methods:
- Tilt-table testing primarily induces symptoms rather than explaining them
- ECG captures only cardiac electrical activity, not autonomic regulation
- Blood pressure measurements provide limited snapshots rather than regulatory patterns
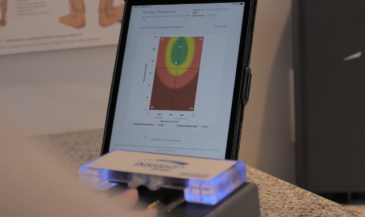
- Heart Rate Variability (HRV) analysis via neuroPULSE technology quantifies autonomic balance and activity
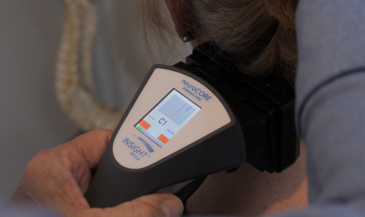
- Surface EMG through neuroCORE assessment reveals patterns of neuromuscular tension affecting posture and movements
- Thermographic scanning with neuroTHERMAL identifies dysautonomia patterns
- Combined metrics create a CORESCORE that provides objective measurement of overall neurological efficiency
Perhaps the most significant difference lies in the management philosophy:
Reactive Symptom Management:
- Wait for episodes to occur, then respond
- Focus on avoiding known triggers
- Medication only for severe cases
Proactive Nervous System Optimization:
- Regular assessment of autonomic function with INSiGHT scanning technology
- Targeted interventions to improve autonomic balance before episodes occur
- Specific care to enhance nervous system resilience and adaptive capacity
Clinical Benefits of Neurological Assessment
Heart Rate Variability (HRV) assessment stands as perhaps the most valuable tool in understanding vasovagal tendencies. The neuroPULSE technology specifically measures what we call the Autonomic Balance Index (ABI) and Autonomic Activity Index (AAI)—key metrics that reveal a patient’s overall adaptive capacity and resilience to stress.
Patients prone to vasovagal episodes often display distinctive patterns in their HRV readings:
- Low overall HRV (reduced adaptability and resilience)
- Exaggerated parasympathetic responses to mild stressors
- Imbalanced sympathetic/parasympathetic ratios, even between episodes
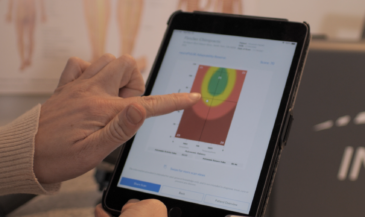
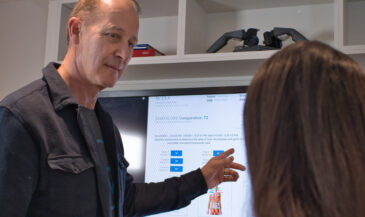
These patterns often appear in what we call the “distressed state” (Zone 3) of the HRV Rainbow Graph—indicating sympathetic dominance with depleted reserves. This state represents a nervous system that lacks the flexibility to appropriately respond to challenges.
The true clinical value of this assessment is its preventative power. By identifying these patterns before an episode occurs, you can initiate care that improves autonomic regulation and builds resilience.
Integrating Neurological Assessment
Start with a comprehensive baseline assessment that includes complete INSiGHT Scanning technology.
The “Rule of 12” approach is particularly effective for patients with vasovagal tendencies:
- 12 initial visits within a condensed timeframe to engage nervous system retraining
- Structured re-assessment at regular intervals (every 12 visits) to track progress
Remember that measurable improvements in autonomic function typically occur within a 12-week window of consistent care. Patients may report fewer prodromal symptoms or an increased ability to abort impending episodes before experiencing objective measurement changes.
Transforming Care Through Neurological Insight
The INSiGHT neuroTECH suite provides the missing piece that conventional approaches lack—objective measurement of nervous system function that can identify susceptibility before episodes occur and track improvements that symptom reporting alone might miss.
The most powerful shift occurs when patients move from seeing themselves as “prone to fainting” to understanding themselves as individuals with measurable autonomic patterns that can be optimized. This change in perspective transforms anxiety about unpredictable episodes into confidence in their improving nervous system function.
By bringing the power of neurological assessment to patients with vasovagal tendencies, you’re not just helping them avoid fainting—you’re offering a pathway to enhanced nervous system regulation that benefits their overall health and wellbeing. That’s the true promise of neurologically-focused care: transforming challenges into opportunities for comprehensive health improvement through better nervous system function.