You know those moments when a patient walks into your office describing sharp, shooting pain that started in their lower back but now radiates down their leg into their foot? They’re confused because what began as a “back problem” has somehow become numbness in their toes and weakness when they try to lift their foot. You likely recognize this as a classic herniated disc presentation, but here’s what’s fascinating—the patient is experiencing something far more complex than simple structural damage.
Herniated discs most often impact people between the ages of 30 and 50, with men being roughly twice as likely to experience them. These injuries most commonly occur in the lumbar and cervical regions of the spine, and while most cases resolve within 2–12 weeks, the journey from symptoms to recovery reveals critical insights about nervous system function that most practitioners overlook.
Here’s what most practitioners miss: Herniated discs aren’t just structural problems requiring structural solutions. The electric, burning sensations that patients describe—the numbness, the weakness, the seemingly random symptoms that appear far from the actual disc injury—these are all neurological manifestations of a nervous system under stress.
Let’s be real—most patients think herniated discs are simply “slipped discs” that need to be “put back in place.” Even many practitioners focus primarily on the structural component, using imaging to confirm the diagnosis and then managing symptoms until the disc tissue hopefully reabsorbs. This approach misses the profound neurological dysfunction that creates the symptoms patients actually experience.
We understand that there’s a more comprehensive story here, one that centers around nervous system function, inflammatory cascades, and the body’s adaptive responses to nerve interference. A herniated disc doesn’t just compress tissue—it creates a complex neurological event that affects everything from pain perception to autonomic function.
With neurologically-focused assessment tools, we can finally measure and track these patterns objectively, transforming how we understand and care for patients experiencing herniated disc symptoms.
The Neurological Foundation of Herniated Disc Symptoms
Understanding herniated disc symptoms requires shifting our perspective from simple mechanical problems to complex neurological events. When the nucleus pulposus pushes through a tear in the annulus fibrosus, it doesn’t just create structural abnormality—it initiates a cascade of inflammatory dysfunction that extends far beyond the immediate area of injury.
The disc nucleus contains proteins and inflammatory chemicals that were never meant to contact nerve tissue. When they leak out, they trigger an inflammatory response that disrupts nerve conduction, sensitizes pain pathways, and interferes with neurological signaling. This explains why patients often experience symptoms that seem disproportionate to what appears on imaging studies.
What makes this particularly fascinating from a neurological perspective is how the body responds systemically to this local injury. The nervous system doesn’t compartmentalize—when one area experiences dysfunction, compensatory patterns develop throughout the entire system. The autonomic nervous system shifts into sympathetic overdrive, affecting sleep, digestion, and even immune response.
The location of disc herniation determines the specific neurological manifestations patients experience:
Cervical Herniations (C5–C8 nerve roots):
• Shoulder blade pain and upper trapezius tension
• Arm pain radiating to specific finger patterns
• Hand numbness affecting grip strength and fine motor skills
Lumbar Herniations (L4–S1 nerve roots):
• Buttocks and posterior thigh pain following dermatome patterns
• Calf pain and potential foot numbness or weakness
• Classic sciatica symptoms with specific nerve root signatures
This neurological mapping helps us understand why a disc problem in the lower back can cause toe numbness, or why a cervical herniation can affect hand function. We’re not just dealing with local tissue damage—we’re managing a nervous system-wide response that demands more than symptomatic relief.
What Herniated Disc Symptoms Actually Feel Like
The symptoms of a herniated disc unfold in predictable patterns that reflect the specific neurological pathways being affected. The most distinctive feature is the electric, shooting quality of the symptoms. Patients often describe sensations that feel like lightning bolts or electrical shocks traveling from the spine into their extremities. This isn’t poetic language—it’s an accurate representation of how irritated nerve tissue transmits signals.
One hallmark symptom that distinguishes disc symptoms from general back tension is that lying down often makes it worse. While most back complaints improve with rest, disc-related nerve irritation frequently intensifies when patients are horizontal—especially at night. Lying flat can increase pressure within the disc and reduce space for inflamed nerve roots.
Key Neurological Manifestations:
- Numbness and tingling in defined patterns
• Muscle weakness—foot drop, grip loss, reduced range
• Coordination issues—trouble buttoning clothes, walking, or writing
Unexpected Symptoms:
Some of the most surprising disc-related signs occur far from the spine. For example, cervical herniations can present like carpal tunnel, and lumbar herniations may mimic circulatory issues in the feet. Patients often report that laughing, coughing, or sneezing trigger sharp flares of discomfort—because increased abdominal pressure pushes on already-irritated structures.
The classic “shock-like” symptom running down one side of the body typically signals sciatic nerve involvement—often with burning, stabbing, or cold sensations following precise anatomical nerve paths.
Traditional Diagnosis vs. Neurological Assessment
When patients present with herniated disc symptoms, the standard approach usually looks like this: take a history, perform an orthopedic test, confirm with imaging. While this method identifies structural issues, it rarely measures the functional impact on the nervous system.
The limitations become obvious when you consider what’s actually causing the suffering. An MRI might show a 4mm bulge at L5–S1, but it won’t show how that interference affects the patient’s stress response, neural adaptability, or compensatory patterns.
The patient’s electric pain, fatigue, sleep disturbances—these are signs of neurological dysfunction that standard tests simply don’t measure.
This is where neurologically-focused scanning makes all the difference. Instead of relying on subjective reporting and structural imaging alone, we can now objectively assess how the nervous system is adapting in real time. Advanced technologies show us patterns that explain why some patients recover quickly while others become chronic.
Clinical Benefits of Neurological Assessment for Herniated Discs
The INSiGHT neuroTECH suite fills in what structural imaging misses—real-time, objective data on how well the nervous system is performing. These assessments go beyond pain relief to reveal the bigger story.
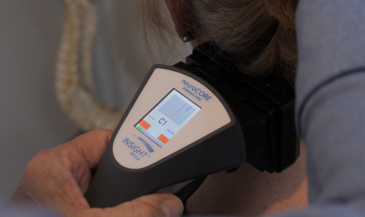
Surface Electromyography (neuroCORE) reveals muscle tone imbalances, showing where hypertonicity or hypotonicity signals energy exhaustion and protective compensation. Research confirms these scans detect secondary tension patterns far beyond the injury site.
Heart Rate Variability (neuroPULSE) shows how inflammation and nerve tension affect autonomic balance. Disc-related stress is frequently reflected in sympathetic overdrive patterns that reduce recovery capacity. The neuroPULSE tracks adaptive reserve, revealing whether a patient’s nervous system has the bandwidth to heal.
Thermal Scanning (neuroTHERMAL) identifies nerve interference by detecting temperature asymmetries, which correlate with inflammation and subluxation patterns. With reproducibility scores between 0.91–0.98, this technology provides clinical precision that patients can trust.
Together, these assessments create the CORESCORE—a single neural efficiency score that simplifies complex findings into a patient-friendly report card.
Implementing Neurologically-Focused Care
Transforming your approach to disc care starts with a full spine nerve system scan using INSiGHT scanning technology. Baseline scans reveal primary and secondary patterns that standard testing misses.
The “Rule of 12” has proven especially effective—12 initial visits over focused timeframes to engage neuroplastic reorganization. Follow-up scans show real neurological progress.
Patient education becomes more powerful when you can visually demonstrate care results. Explaining how disc symptoms affect neurological balance—and showing that improvement on a scan—creates buy-in that lasts.
Multiple studies confirm that chiropractic adjustments can positively influence heart rate variability and autonomic function. When patients see progress in their adaptability—not just symptom relief—they stay engaged.
Elevating Herniated Disc Care Through Neurological Excellence
When we look at herniated discs through a neurological lens, everything shifts. This isn’t just about structure—it’s about how well the nervous system can adapt and recover.
INSiGHT scanning offers a way to objectively show progress, helping patients move from fear to empowerment. With care guided by real data—not guesswork—you can demonstrate outcomes that go far beyond symptom relief.
Let’s stop managing symptoms and start measuring adaptation. That’s where neurologically-focused chiropractic care excels. That’s where we truly make a difference.