By Dr. Christopher Kent
Affixed surface electrodes may be employed for real time assessment of paraspinal muscle activity throughout ranges of motion. The author has developed a protocol for the dynamic assessment of paraspinal muscle activity in chiropractic practice.
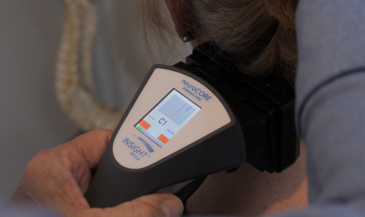
A two channel computerized EMG scanner is used in conjunction with pre-gelled disposable, self-adhesive electrodes. The skin of the patient is prepared with an alcohol wipe, and dried. Active electrodes are placed at like points on each side of the paravertebral skin. Upper and lower active electrodes are employed. A ground reference electrode is placed over a bony prominence on the wrist of the patient. Shielded cables are used between the active electrodes and the instrument to minimize induced noise.
The patient is instructed to execute the specific motion being examined while a five-second acquisition of EMG signal is obtained. The relative levels of EMG activity are then plotted on an amplitude/time X-Y graph. A baseline graph is recorded with the patient in the neutral position.
The flexion relaxation phenomenon
Allen observed that when the trunk is flexed, the lumbar paraspinal muscles exhibit EMG activity as eccentric contraction controls trunk lowering. However, when the end range of lumbar flexion is reached, the lumbar paraspinal muscles exhibit electrical silence. This is believed to be a result of lumbar spine support by posterior ligamentous structures rather than active muscles.[1]
Floyd and Silver and Pauley suggested that the erector spinae muscles are more active in extension than in flexion. These investigators noted the phenomenon of electrical silence in the erector spinae muscles during full trunk flexion. [2,3,4]
Wolf et al observed EMG silence might occur when trunk flexion exceeded 70 degrees and reported that such relaxation occurred most commonly between 80-90 degrees. EMG activity usually resumed after 20 degrees of extension from the fully flexed trunk position, but occurred anywhere from 90-30 degrees of flexion. [5]
Floyd and Silver reported that in patients experiencing “back-ache,” the flexion relaxation phenomenon was absent.
In addition, Triano and Schultz found that presence or absence of the flexion relaxation phenomenon was related to scores on the Oswestry low back pain questionnaire. They concluded, “These findings imply that myoelectric signal levels, trunk strength ratios, and ranges of trunk motion may be used as objective indicators of low-back pain disability.” [6]
Ahern et al investigated the reliability of lumbar paravertebral surface EMG in a sample of 70 patients with chronic low back pain. [7]
Patients were evaluated in the standing and seated positions. SEMG was also performed during flexion/extension, rotation, walking, and stooping. These authors calculated a flexion extension index by subtracting the minimum from the maximum EMG values occurring at maximum flexion. Rotation indices, representing the difference between right and left EMG at maximal rotation were also determined. Within session reliability was calculated using Pearson’s r. Coefficients ranged from 0.66 to 0.97.
In another study, Ahern et al compared the lumbar paravertebral SEMG patterns in chronic low back pain patients with those of non-patient controls. They found significant differences between groups on low back muscle activity during dynamic movements. Such differences were not observed using static postures. [8]
Meyer et al examined 10 subjects to see if the flexion relaxation phenomenon was also present in the cervical spine. Surface electrodes were placed parallel to the cervical paraspinal muscles, and EMG activity was recorded as the patient was instructed to flex the cervical region. The investigators noted that in the cervical spine, end range of motion occurs after full forward flexion. It was concluded that cervical paraspinal muscles exhibit a flexion relaxation pattern similar to that which occurs in the normal lumbar spine. Full-flexion relaxation was observed in all 10 asymptomatic subjects. [9]
Lateral flexion and rotation
Dolce and Raczynski reported that during lateral flexion (side bending) the erector spinae muscles demonstrate increased activity on the contralateral side. [10]
Wolfe et al found that during rotation, increased paraspinal muscle activity occurs on both sides. The side contralateral to the direction of rotation displays significantly more activity than the ipsilateral side. These studies, however, were limited to the lumbar paraspinal muscles. [5]
Donaldson and Donaldson and Cram employed dynamic SEMG examinations as outcome assessments for biofeedback therapy. These examinations included flexion, extension, lateral bending, and rotation, and were not confined to the lumbar region. [11,12,13]
Donaldson and Donaldson examined 276 persons in pain (200 clinical patients and 76 research subjects) and reported that in 97.5% of these cases, a 20% or greater imbalance was measured. Examination of a control group of 40 non-pain subjects found asymmetries ranging from 5% to 10%.
Furthermore, Donaldson and Donaldson described two “rules” which they used to discriminate between pain and non-pain patients:
1. In non-pain subjects symmetrical movement produces symmetrical patterns.
2. In pain patients symmetrical movement produces asymmetrical patterns.
Thus, it appears that dynamic SEMG studies may have clinical utility in discriminating between pain and non-pain populations. To the chiropractor, however, there are several significant shortcomings to pain-based models for outcome assessment:
- Such schemes assume that the objective of chiropractic care is symptomatic treatment of pain;
- Pain is a highly subjective, private sensation which cannot be directly measured or observed;
- In some instances, unless the pain is robust enough to restrict activities of daily living, a “false negative” could result;
- Pain criteria cannot be applied if the patient has symptoms other than pain, or no symptoms at all; and
- Pain criteria are useless in the evaluation of asymptomatic patients undergoing maintenance or reconstructive care. [14]
If the objective of chiropractic care is the correction of vertebral subluxations, criteria must be developed which reliably evaluate their presence and correction. Alterations in spinal mobility and asymmetrical muscular activity are generally recognized manifestations of vertebral subluxation. [15,16]
Therefore, dynamic SEMG studies may be useful in analyzing subluxations as well as discriminating between pain and non-pain populations.
Indications for dynamic assessment
Gentempo and Kent have published specific indications for static surface EMG scanning. [17]
They maintain that the static, full spine, seated study is the initial SEMG examination of choice, and should precede any dynamic assessments. The value of dynamic assessment is that it may reveal abnormalities which are not disclosed on the static examination. Therefore, when the static scan fails to disclose abnormality in the region(s) of clinical interest, dynamic assessment may be employed for further characterization of the myodynamics of the patient.
Follow up examinations should be performed to evaluate patient response to chiropractic care. Generally, such follow up studies would be performed as part of regular re-exams, typically at 10-12 visit intervals. Follow up exams are indicated until the patterns normalize, or maximal improvement is attained. Equivocal subluxation findings, an exacerbation of the patient’s condition, or a new illness or injury justify reevaluation of clinical need for the test.
Interpretation of patterns
In chiropractic practice, the primary purpose of SEMG procedures is the quantitative assessment of subluxation-related paravertebral muscle activity. It must be emphasized that SEMG is not a “stand alone” diagnostic technique for a specific clinical entity. Rather, it is a measurement which, when taken in concert with other examination findings, is useful in chiropractic analysis.
Interpretation procedures for dynamic assessments differ from those for static scans. Normative data have been developed for static scans. Interpreting dynamic scans involves different criteria. In flexion, our primary interest is the presence or absence of flexion relaxation, as well as symmetry. In extension, symmetry should be maintained. In rotation and lateral flexion, we examine for a “mirror imaging” of SEMG signal [14].
Conclusion
Dynamic paraspinal SEMG techniques provide reliable information concerning the activity of paraspinal muscles during movement. This information may be used by the chiropractor in analyzing structure- function relationships associated with the vertebral subluxation.
References
1. Allen C: “Muscle action potentials used in the study of dynamic anatomy.” Br J Phys Med 1948;11:66.
2. Floyd WF, Silver P: “The function of the erector spinae muscles in certain movements and postures in man.” J Physiol (Lond) 1955;129:184.
3. Floyd WF, Silver P: “Function of the erector spinae in flexion of trunk.” Lancet 1951;1:133.
4. Pauly J: “An electromyographic analysis of certain movements and exercises I. Some deep muscles of the back.” Anat Rec 1966 155:223.
5. Wolf SL, Basmajian JV, Russe TC, Kutner M: “Normative data on low back mobility and activity levels.” Am J Phys Med 1979;58(5):217.
6. Triano JJ, Schultz AB: “Correlation of objective measure of trunk motion and function with low-back disability ratings.” Spine 1987;12(6):561.
7. Ahern DK, Follick MJ, Council JR, Laser-Wolston N: “Reliability of lumbar paravertebral EMG assessment in chronic low back pain.” Arch Phys Med Rehabil 1986;67:762.
8. Ahern DK, Follick MJ, Council JR, Laser-Wolston N, Litchman H: “Comparison of lumbar paravertebral EMG patterns in chronic low back pain patients and non-patient controls.” Pain 1988;34:153.
9. Meyer JJ, Anderson AV, Berk RJ: “The flexion-relaxation henomenon: does it exist in the cervical spine?” Proceedings of the 1990 international conference on spinal manipulation. FCER, Arlington, VA.
10. Dolce JJ, Raczynski JM: “Neuromuscular activity and electromyography in painful backs: psychological and biomechanical models in assessment and treatment.” Psychological Bull 1985;97(3):502-520.
11. Donaldson S, Donaldson M: “Multi-channel EMG assessment and treatment techniques.” In Cram J (ed) “Clinical EMG for Surface Recordings: Volume 2.” Clinical Resources. Nevada City, CA. 1990.
12. Cram J: “Clinical EMG: muscle scanning for surface electrodes.” Biofeedback Institute of Seattle. Seattle, WA, 1986.
13. Cram J: “EMG muscle scanning and diagnostic manual for surface recordings.” In Cram J (ed) “Clinical EMG for Surface Recordings: Volume 2.” Clinical Resources. Nevada City, CA. 1990.
14. Kent C, Gentempo P: “Dynamic paraspinal surface EMG: a chiropractic protocol.” Chiropractic Research Journal 1993 2(4): 40.
15. Janse J, Houser RH, Wells BF: “Chiropractic Principles and Technic.” National College of Chiropractic. Chicago, IL. 1947 (reprinted 1978).
16. Schafer RC: “Basic Chiropractic Procedural Manual.” American Chiropractic Association. Arlington, VA. 1984.
17. Gentempo P, Kent C: “Establishing medical necessity for paraspinal EMG scanning.” Journal of Chiropractic Research, Study, and Clinical Investigation 1990 3(1):22.