By Dr. Christopher Kent
Objective analysis of vertebral subluxations in children poses a challenge to many chiropractors.
As Lantz (1) noted, “Common to all concepts of subluxation are some form of kinesiologic dysfunction and some form of neurological involvement.”
A review of models of vertebral subluxation has been published elsewhere.(2) However, regardless of the elegance of a theoretical model, it must be capable of being made operational if it is to be used to develop clinical strategies.
Doctors of chiropractic who provide care to infants and children seek assessment procedures which — while providing objective, quantifiable information — are non-invasive, cost-effective, and practical.
The three-dimensional (3-D) model was developed as an initial step in the operational definition of vertebral subluxation. It incorporates traditional chiropractic constructs, and serves as a bridge to contemporary technology. It incorporates clinical assessments which may be applied to persons of any age.
The 3-D model of vertebral subluxation has three components. Each component may be reliably measured using appropriate instrumentation. These measurements provide objective evidence concerning manifestations of vertebral subluxation. The three components are:
1. Dyskinesia. Dyskinesia refers to distortion or impairment of voluntary movement.(3) Spinal motion may be reliably measured using inclinometry.(4) Alterations in regional ranges of motion may be associated with vertebral subluxation.(5)
2. Dysponesis. Dysponesis is evidenced by abnormal tonic muscle activity. Dysponesis refers to a reversible physiopathologic state consisting of errors in energy expenditure, which are capable of producing functional disorders. Dysponesis consists mainly of covert errors in action potential output from the motor and premotor areas of the cortex and the consequences of that output. These neurophysiological reactions may result from responses to environmental events, bodily sensations, and emotions. The resulting aberrant muscle activity may be evaluated using surface electrode techniques.(6) Typically, static SMEG with axial loading is used to evaluate innate responses to gravitational stress.(7) Dysponesis may also be disclosed by postural analysis.
Pediatric data
Surface EMG potentials in children are higher than those of adults. Gentempo and Kent (8) published a study evaluating 14 children, 2 to 14 years of age. The mean age was 6.4 years (SD=3.2). Six boys and eight girls were examined. The number of chiropractic office visits prior to the EMG exam ranged from 2 to 48 (mean=16.8, SD=14.3). The mean, standard deviation, and median were calculated for each of the 30 paraspinal sites evaluated. The minimum reading, maximum reading, and range were also obtained. SEMG potentials in children were found to be significantly higher than those of adults.
SEMG patterns
In the interpretation of pediatric SEMG scans, two factors are considered:
A) Amplitude — referring to the signal level in microvolts. The higher the signal level, the greater the extent of the paraspinal muscle activity. Focal areas of altered muscle activity may be identified.
B) Symmetry — referring to a comparison of the left side to the right side.
Paraspinal EMG scans, taken in concert with other examination findings, may be helpful in determining the following:
- Asymmetrical contraction
- Areas of muscle splinting
- Severity of the condition
- Aberrant recruitment patterns
- Dysponesis
- Responses to dysafferentation
- Response to chiropractic adjustment
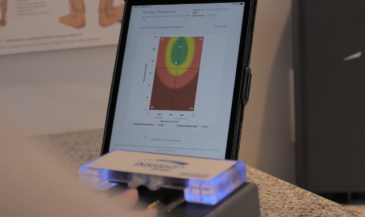
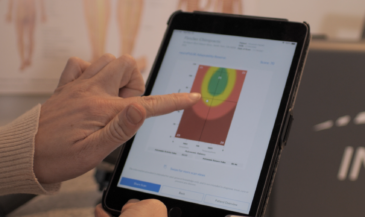
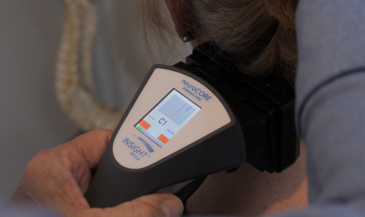
3. Dysautonomia. The autonomic nervous system regulates the actions of organs, glands, and blood vessels. Acquired dysautonomia may be associated with a broad array of functional abnormalities.(9,10,11,12,13,14) Autonomic dystonia may be evaluated by measuring skin temperature differentials.(15) Uematsu et al (16) determined normative values for skin temperature differences based upon asymptomatic “normal” individuals. The authors stated, “These values can be used as a standard in assessment of sympathetic nerve function, and the degree of asymmetry is a quantifiable indicator of dysfunction… Deviations from the normal values will allow suspicion of neurological pathology to be quantitated and therefore can improve assessment and lead to proper clinical management.” Skin temperature differentials are associated with vertebral subluxation.(17)
B.J. Palmer developed and used a system of skin temperature analysis called the “pattern system.” Miller (18) described the basic premise of pattern analysis as follows:
“Persons free of neurological interference tend to display skin temperature readings which continually change, but when the vertebral subluxation and interference to normal neurological function appear on the scene, these changing differentials become static. They no longer display normal adaptability, and at this time the patient is said to be `in pattern.’”
Clinical observations from users suggest the following:
- In normal (unsubluxated) patients, thermal patterns will be constantly changing, and will exhibit acceptable symmetry.
- In acute and subacute subluxations, there will be levels out of range, but the pattern will vary.
- In chronic subluxations, the pattern will be fixed, and there will be levels out of range.
- Levels of asymmetry often do not relate to the level of primary subluxation.
- Chronic organ dysfunction (visceroautonomic) may result in a focal segmental asymmetry.
- Thermal patterns measure autonomic activity. Levels of thermal asymmetry may not correlate with levels of EMG asymmetry, since EMG is measuring muscle activity, not autonomic function.
These observations should be tested through formalized research. The chiropractic profession pioneered skin temperature differential analysis with the introduction of the neurocalometer more than 70 years ago. Strengthened by extensive clinical experience and ongoing research, paraspinal skin temperature differential analysis is strongly established in the practice of subluxation based chiropractic.(17)
Conclusion
This three-dimensional model may be used with any technique, which has as its objective the detection, management, or correction of vertebral subluxation. Correction of vertebral subluxation facilitates the restoration of proper tone throughout the nervous system.
Health is dependent upon maintaining appropriate tone in the nervous system. As D.D. Palmer explained: “Life is action governed by intelligence. Intelligent life, the soul, depends upon the execution of functions. Functions performed by normal energy is health. Disease is the result of the performance of functions above or below a normal degree of activity. Impulses properly transmitted through nerves, result in functions being normally performed, a condition which results in health.”(19)
The ability to maintain tone requires a nervous system free of interference. Restoration of tone is dependent upon correction of vertebral subluxations. Alterations in the tone of the somatic system may be objectively evaluated using surface EMG. Altered autonomic tone may be evaluated using skin temperature measurements. Changes in ranges of motion may be measured to assess dyskinesia. Such objective assessments have the potential to make chiropractic the dominant strategy of 21st century health care.
References
1. Lantz CA: “The subluxation complex.” In: Gatterman MI (ed): “Foundations of Chiropractic Subluxation.” Mosby, St. Louis, MO, 1995.
2. Kent C: “Models of vertebral subluxation: a review.” Journal of Vertebral Subluxation Research 1996;1(1):11.
3. “Dorland’s Pocket Medical Dictionary.” 25th edition. WB Saunders Company. 1995.
4. Saur PM, Ensink FB, Frese K, et al: “Lumbar range of motion: reliability and validity of the inclinometer technique in the clinical measurement of trunk flexibility.” Spine 1996;21(11):1332.
5. Blunt KL, Gatterman MI, Bereznick DE: “Kinesiology: an essential approach toward understanding the chiropractic subluxation.” Chapter 11. In: Gatterman MI (ed): “Foundations of Chiropractic Subluxation.” Mosby, St. Louis, MO. 1995.
6. Whatmore GB, Kohi DR: “Dysponesis: a neurophysiologic factor in functional disorders.” Behav Sci 1968;13(2):102.
7. Kent C: “Surface electromyography in the assessment of changes in paraspinal muscle activity associated with vertebral subluxation: a review.” Journal of Vertebral Subluxation Research 1997;1(3):15.
8. Kent C, Gentempo P: “Paraspinal EMG potentials in pediatric patients: preliminary observations.” Chiropractic Research Journal 1992; 2(2):48.
9. Backonja M-M: “Reflex sympathetic dystrophy/sympathetically mediated pain/causalgia: the syndrome of neuropathic pain with dysautonomia.” Seminars in Neurology 1994;14(3):263.
10. Goldstein DS, Holmes C, Cannon III RO, et al: “Sympathetic cardioneuropathy in dysautonomias.” New Engl J Med 1997;336(10):696.
11. Vassallo M, Camilleri M, Caron BL, Low PA: “Gastrointestinal motor dysfunction in acquired selective cholinergic dysautonomia associated with infectious mononucleosis.” Gastroenterology 1991;100(1):252.
12. Baron R, Engler F: “Postganglionic cholinergic dysautonomia with incomplete recovery: a clinical, neurophysiological and immunological case study.” J Neurol 1996;243:18.
13. Soares JLD: “Disautonomias.” Acta Medica Portuguesa 1995;8(7-8):425. Written in Portuguese. English abstract.
14. Stryes KS: “The phenomenon of dysautonomia and mitral valve prolapse.” J Am Acad Nurse Practitioners 1994;6(1):11.
15. Korr IM. “The Collected Papers of Irvin M. Korr.” American Academy of Osteopathy. Indianapolis, IN. 1979.
16. Uematsu S, Edwin DH, Jankel ER, et al: “Quantification of thermal asymmetry.” J Neurosurg 1988;69:552.
17. Kent C, Gentempo P: “Instrumentation and imaging in chiropractic: a centennial retrospective.” Today’s Chiropractic 1995;24(1):32.
18. Miller JL: “Skin temperature differential analysis.” International Review of Chiropractic (Science) 1964;1(1):41.
19. Palmer DD: “Text-book of the Science, Art and Philosophy of Chiropractic for Students and Practitioners.” Portland Printing House Company. Portland, OR. 1910. Page 661.
(Dr. Christopher Kent, president of the Council on Chiropractic Practice, is a 1973 graduate of Palmer College of Chiropractic. The WCA’s “Chiropractic Researcher of the Year” in 1994, and recipient of that honor from the ICA in 1991, he was also named ICA “Chiropractor of the Year” in 1998. Dr. Kent is director of research for EMG Consultants, Inc., and a co-founder of Paradigm Partners, Inc. and the Chiropractic Leadership Alliance. With Dr. Patrick Gentempo, Jr., Dr. Kent produces a monthly audio tape journal, “On Purpose,” covering current events in science, philosophy, and politics of vital interest to the practicing chiropractor. For subscription information call 800/892-6463.)