Alterations in skin temperature patterns are associated with aberrations in the function of the autonomic nervous system.
The autonomic nervous system controls the organs, glands, and blood vessels. It is responsible for relating the internal environment of the patient to the dynamics of the outside world. One important function of the autonomic nervous system is temperature regulation.
When the outside environment is cool, the body will attempt to conserve heat, resulting in constriction of the arterioles in the skin. When the outside environment is warm, and the body seeks to eliminate heat, vasodilation of the arterioles in the skin will result. (1)
In a healthy patient, skin temperature patterns will be constantly changing, but symmetrical. This is because a healthy body is constantly adapting to the environment.
Vertebral subluxations result in thermal asymmetries and/or fixed patterns. The levels of thermal asymmetry are not necessarily the levels of subluxation, and may change with time. The value of the thermal scan is in determining the overall degree of autonomic abnormality, and the response of the patient to the adjustment.
Two mechanisms have been proposed which relate to altered skin temperatures, the segmental and the nonsegmental.
The segmental model
According to the segmental model, sensory irritation via the recurrent meningeal nerve may result in a sympathetic response of vasoconstriction. This will produce thermal asymmetry in the “thermatome” affected.
A thermatome is similar to a dermatome, but refers to a region of temperature change rather than sensation. When this mechanism is operative, the level of the thermal asymmetry is often the same as the level of subluxation, or is close to it.
Some clinicians report that chronic subluxations or long standing organic disease may be associated with segmental responses. Segmental facilitation of the lateral horn cells of the spinal cord may produce similar changes.
The nonsegmental model
Sensory innervation of the intervertebral discs and facet joints is not only segmental, but is also nonsegmental through the paravertebral sympathetic trunk. Therefore, a subluxation at any level of the spine may produce thermal changes throughout the entire spine. Depending up on the degree of chronicity, these changes may be fluctuating or “fixed” into a pattern.
Clinical analysis
In the analysis of thermal differentials, we are concerned with two factors, symmetry and pattern.
Symmetry refers to the difference in temperature between the left side at the right side at like points along the spine. It has been demonstrated that specific temperatures vary greatly from person to person. Actual temperatures also vary in the same person from moment to moment. However, the differences in temperature from side to side are maintained within strict limits in healthy persons.
Uematsu et al determined normative values based upon 90 asymptomatic “normal” individuals. These authors stated: “These values can be used as a standard in assessment of sympathetic nerve function, and the degree of asymmetry is a quantifiable indicator of dysfunction…Deviations from the normal values will allow suspicion of neurological pathology to be quantitated and therefore can improve assessment and lead to proper clinical management.” (2)
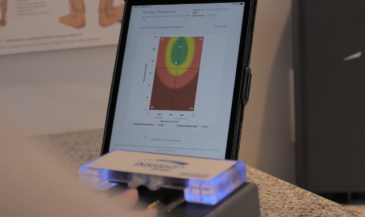
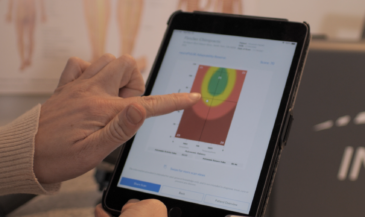
These values have been incorporated into the Insight 7000 software. Mild, moderate, and severe asymmetries are identified by color bars. Temperature differences between one and two standard deviations indicate a mild asymmetry; two to three standard deviations a moderate asymmetry; while three or more are indicative of a severe asymmetry.
It must be remembered that since vasomotor activity should be a dynamic process, the levels of asymmetry will change from session to session unless a chronic subluxation is present. Even though the levels change, a patient with acute or subacute subluxation will usually have approximately the same number of levels out of range, although the levels themselves may change.
The thermal sensors, when properly used, provide excellent reliability (reproducibility) of temperature measurement. However, temperature patterns on a patient change from moment to moment unless chronic subluxation is present. This may incorrectly lead the examiner to believe that the instrument or procedure is not reproducible. Reproducible readings indicate chronic subluxation. This is NOT a normal or desirable state of affairs.
Patterns
B.J. Palmer developed and used a system of skin temperature analysis called the “pattern system.”
Miller described the basic premise of pattern analysis as follows:
“Persons free of neurological interference tend to display skin temperature readings which continually change, but when the vertebral subluxation and interference to normal neurological function appear on the scene, these changing differentials become static. They no longer display normal adaptability, and at this time the patient is said to be `in pattern.’” (3)
Clinical observations from users suggest the following:
1. In normal (unsubluxated) patients, thermal patterns will be constantly changing, and will exhibit acceptable symmetry.
2. In acute and subacute subluxations, there will be levels out of range, but the pattern will vary.
3. In chronic subluxations, the pattern will be fixed, and there will be levels out of range.
4. Levels of asymmetry often do not relate to the level of primary subluxation.
5. Chronic organ dysfunction (visceroautonomic) may result in a focal segmental asymmetry.
6. Thermal patterns measure autonomic activity. Levels of thermal asymmetry may not correlate with levels of EMG asymmetry, since EMG is measuring muscle activity, not autonomic function.
These observations should be tested through formalized research. The chiropractic profession pioneered skin temperature differential analysis with the introduction of the neurocalometer over 70 years ago. Strengthened by extensive clinical experience and ongoing research, paraspinal skin temperature differential analysis is strongly established in the practice of subluxation based chiropractic. (4)
References
1. “Segmental Neuropathy.” Canadian Memorial Chiropractic College. Toronto. No date.
2. Uematsu S, Edwin DH, Jankel ER, et al: “Quantification of thermal asymmetry.” J Neurosurg 1988;69:552.
3. Miller JL: “Skin temperature differential analysis.” International Review of Chiropractic (Science) 1964;1(1):41.
4. Kent C, Gentempo P: “Instrumentation and imaging in chiropractic: a centennial retrospective.” Today’s Chiropractic 1995;24(1):32.