Let me tell you something I’ve learned over the years: most people want to stick with chiropractic. They just don’t know what they’re sticking with.
Patients come in because of symptoms, but if you don’t provide a clear plan for what comes next, they’ll often leave as soon as those symptoms improve.
That’s why I developed a framework called “The Rule of 12.” It gives structure to your care plans and a practical, measurable way to keep patients engaged—not just for 12 visits, but for 12 weeks, 12 months, and beyond. When paired with INSiGHT scanning technology and the CORESCORE neurological report card, this framework turns early trust into long-term commitment.
When you give people a plan—and you show them that their nervous system is changing—you build the kind of trust that keeps families under care for years.
And you don’t need a complicated protocol to make it happen. You need a plan with rhythm. A system that aligns with the science of neurological change… and one that makes sense to real folks.
That’s what the Rule of 12 does.
Care Planning Needs Structure Patients Can Understand
Retention isn’t just a business metric—it’s the heartbeat of a thriving chiropractic practice. When patients commit to ongoing care, it means they’ve moved beyond reacting to symptoms and into a mindset of sustained neurological optimization. But commitment doesn’t happen by accident. It happens when your patients are guided—not just adjusted.
Most patient drop-offs don’t occur because care isn’t working. They happen because patients aren’t clear on what they’re committing to—or why it matters.
The Rule of 12 solves that.
By establishing a predictable sequence—12 initial visits with progress and comparative re-exams built into the first 12 weeks, expanding into 12 months of ongoing restorative care—you give patients a simple, digestible roadmap for their healing journey. It’s the classic answer to the question: How do you eat an elephant? Answer: One bite at a time.
Rather than overwhelming new patients with an open-ended commitment, the Rule of 12 gives them a first milestone they can wrap their minds around. That initial 12-visit segment becomes the critical foundation to observe how well their nervous system is adapting under care.
This structure removes confusion. It shows patients what they’re committing to—and why it matters.
Click here to watch our Rule Of 12 webinar.
The First 12: Building the Foundation
The first 12 visits serve a dual purpose: they initiate neurological changes and set the rhythm for future care and they typically address the issues that brought the patient to your office. By the end of this initial sequence, you’re ready to rescan and re-evaluate. In the Rule of 12, re-exams are the critical foundation for shifting the outcome conversation away from symptoms towards function and performance. These re-exams become the road signs on a map of their future neuro-spinal health. This first progress scan isn’t just for you—it’s a visual and objective confirmation for the patient that care is making a measurable difference.
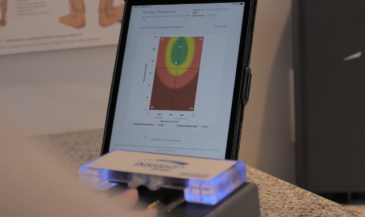
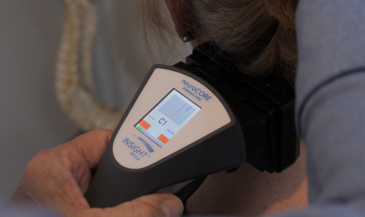
At this stage, you’ll deliver an updated CORESCORE report, which combines data from the neuroTHERMAL, neuroCORE, and neuroPULSE instruments to provide a snapshot of nervous system performance. This Progress Report describes the improvements and changes that you can have analyze=d. In most cases, the deeper embedded habits within the nervous system have to be unwound before new and healthier patterns can replace them. This is where the CORESCORE shines—it helps the patient see the change, and that visibility confirms their path and creates momentum.
The Next 12: Establishing New Patterns
After the first 12 visits, you expand the lens toward a 12-week outcome. Why 12 weeks?
Because neuroplasticity takes time. The nervous system doesn’t just respond to one adjustment—it reprograms through consistency and repetition. In these first 12 weeks, you start to see the trends. You’ll be scanning every 12 visits, building a portfolio of change for each and every patient. From Progress Exams to Comparative exams, you’ll begin to track patterns deep within the nervous system. You’ll be watching neuroplasticity in living color!. And with each scan, you have another opportunity to connect the dots between what the patient is feeling—and what their nervous system is actually doing.
Whether you’re adjusting 3x/week or 4x/month, the key is this: every 12 visits includes a scan. Every scan includes a report. Every report is a chance to reinforce the value of care and deepen the patient’s trust.
The Long Game: 12 Months and Beyond
Once neurological adaptability starts trending upward and the patient has experienced care across 12 visits and 12 weeks, you now have the context to map out their performance-based future.
Twelve months becomes the new anchor. This isn’t just about maintenance—it’s about performance and potential elevation. You’re helping the patient stabilize their system, optimize their adaptability, and expand their capacity for life.
And you’re doing it with data—not guesswork. Each 12-visit checkpoint provides new insights, new conversations, and new opportunities to guide the patient into a lifestyle built around a well-adjusted nervous system.
Some may go on for 12 years. But it all starts with the first 12.
Scans That Motivate. Reports That Retain.
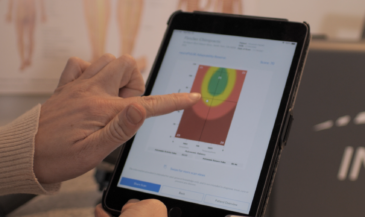
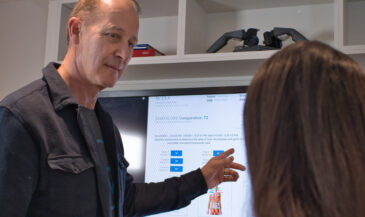
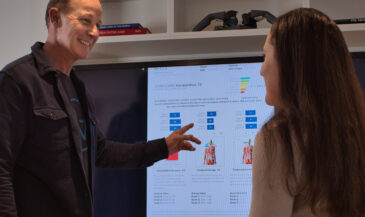
What makes this framework so effective is how it integrates scanning into care. You’re not just making clinical decisions—you’re showing patients their transformation.
You’ll see HRV rise into the Green Zone, signaling recovery and reorganizational capacity. . You’ll watch sEMG go from high-tension patterns to calm postural balance. You’ll see thermal scans release older patterns and continue tostabilize and normalize. And every time, you’ll deliver a new CORESCORE report that shows how far they’ve come—and what’s possible next.
This is what builds retention: visible change, explained clearly, anchored to a care plan with structure.
Why the Rule of 12 Works
Let’s recap what makes this care planning method so powerful:
- It’s simple: Patients can grasp the idea of 12 visits. It’s not abstract. It’s not indefinite.
- It’s strategic: Each cycle corresponds to neurological adaptation timelines and meaningful scan intervals. Neuroplastic change requires time, consistency, and checkpoints.
- It’s measurable: You’re integrating INSiGHT scans at every checkpoint to track real changes in adaptability, posture, and autonomic regulation.
- It gives structure to your care plans: Each phase—12 visits, 12 weeks, 12 months—builds logically on the one before it.
- It builds retention by creating rhythm: Every 12 visits comes with a scan, a conversation, and a renewed plan.
- It keeps patients motivated with data: Each CORESCORE update becomes a progress milestone.
- It’s simple to communicate: Patients can easily understand and commit to this approach.
The Rule of 12 Creates Lifelong Patients
The more neurological scans I’ve seen—the more I’ve realized just how powerful an organized care plan, basd on objective data little structure can be. The Rule of 12 gives you something simple, natural, and neurologically sound to build your care plans around. It helps your patients feel like they’re on a journey with clear roadsignscheckpoints, not just showing up for another visit. And when you combinepair that rhythm with INSiGHT scans and the CORESCORE, well… now you’ve got something people can see and understand. believe in.
When patients understand their care plan—and see their progress along the way—they don’t quit. They keep showing up. They bring their family. They refer their friends. And they begin to see chiropractic not as a quick fix, but as a long-term strategy for nervous system performance.
That’s the power of the Rule of 12.
It helps you deliver care with clarity. It gives patients a roadmap they can follow. And it turns every INSiGHT scan into an opportunity to re-engage, re-educate, and re-commit.
So if you’re looking to boost retention, simplify your care planning, and create more “aha!” moments with your patients, I can’t recommend the Rule of 12 enough. It’s not just good for business—it’s good for the nervous system. And when the nervous system’s happy, everything else starts working better too. Keep scanning, keep leading, and keep showing your community what true, measurable health looks like—one 12-visit step at a time.
Want even more examples of how you can implement the Rule of 12 in your practice? Click here to watch our Rule Of 12 webinar.
If now is the right time for you to explore the advantages of INSiGHT scanning while applying the Rule of 12, get in touch with an INSiGHT advisor. They can walk you through the steps of integrating INSiGHT scanning into your practice, so you can begin to share the power of chiropractic care using objective data and compelling reports. Click here to book a no-obligation call.